To Add is Expected, To Subtract is Design
A couple years ago I wrote about how healthcare should take customer experience guru Dan Gingiss’s advice: do simple better. Now new research illustrates why this is so hard: when it comes to trying to make improvements, people would rather add than subtract.
That, in a nutshell, may help explain why our healthcare system is such a mess.
The research, from University of Virginia researchers, made the cover of last week’s Nature, under the catchy title Less Is More. Subjects were given several opportunities to suggest changes to something, such as a Lego set-up, a geometric design, an essay or even a travel itinerary. The authors found: “Here we show that people systematically default to searching for additive transformations, and consequently overlook subtractive transformations.”
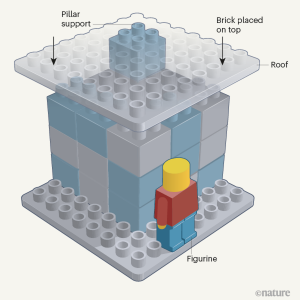
In the Lego picture here, for example, when asked how to strengthen the upper platform, most people wanted to add new columns, instead of simply removing the existing column. The researchers note: “The subtractive solution is more efficient, but you only notice it if you don’t jump to an additive conclusion.”
Giving cognitive nudges – like explicitly mentioning the option of deleting something – improved the likelihood that people would come up with subtractive options, but increasing cognitive load (through additional tasks) decreased it. Co-author Benjamin Converse said:
“Additive ideas come to mind quickly and easily, but subtractive ideas require more cognitive effort. Because people are often moving fast and working with the first ideas that come to mind, they end up accepting additive solutions without considering subtraction at all.”
Leidy Klotz, one of the authors, told Technology Networks:
…just think about your own work and you will see it. The first thing that comes to our minds is, what can we add to make it better. Our paper shows we do this to our detriment, even when the only right answer is to subtract. Even with financial incentive, we still don’t think to take away.
“Overlooking subtraction may mean that people are missing out on opportunities to make their lives more fulfilling, their institutions more effective and their planet more livable,” the team wrote.
In a companion Nature paper, NYU professors Mayvis and Yoon have an interesting explanation: “we propose that the bias towards additive solutions might be further compounded by the fact that subtractive solutions are also less likely to be appreciated. People might expect to receive less credit for subtractive solutions than for additive ones.”
They also speculate that subtractive solutions “might feel less creative,” that “people could assume that existing features are there for a reason,” and that the sunk cost bias is strong.
I think they may be on to something.
Generally speaking, people don’t get paid for removing features. They don’t get applause for eliminating jobs. And they rarely get promoted for telling their bosses they’ve been wasting their money. Much safer to propose something new, which is almost always additive.
Our healthcare system is like a living archaeological site, with layers upon layers of history. We have email but we still have faxes. We have digital ultrasound but we still have X-rays. We have electronic records but we still have plenty of paper. Doctors still wear lab coats because, well, some surgeons in the 19th century thought it was a good idea.
The ABMS has – count ‘em! – 40 specialties and 87 subspecialities for physicians, who might be M.D.s or D.O.s. That doesn’t include other non-physician medical specialties whose practitioners also refer to themselves as “doctor,” such as PharmD, DPM, DDS, DMD, DPT, AuD, or certain Ph.D.s.
We have emergency rooms, free-standing emergency rooms, and urgent care centers. We have surgical centers and freestanding ambulatory surgical centers. We have in-person doctor visits and telehealth doctor visits.
We have for-profit and non-profit hospitals, health plans, nursing homes, and home health agencies, although you couldn’t predict the amount of profit earned just by the type they claim to be. At least pharmaceutical companies and medical device manufacturers are honest about their goals.
Digital health is exploding, with scores of new companies and record-setting amounts of funding for them. Most offer point solutions for specific problems/populations.
We created employer-sponsored health insurance to get around wage controls in the 1940’s, and just kept it when they went away. We created Medicare and Medicaid in the 1960’s and tweaked them ever since, while adding related programs like CHIP. We have the Veteran’s Health Administration and the Military Health System, not to mention the Public Health Service, federally qualified health centers, and the National Health Service Corps.
We have health insurance, both public and private, but we also have health coverage through workers compensation and auto insurance, plus dental and vision coverage. People on Medicare usually have Parts A, B, and D, plus a supplement, or may have a Medicare Advantage plan. I’ve lost count of how many health-related IDs and portals I have.
Comments
Post a Comment